(First, please check our video posted in October 2023 on "Cluneal nerve entrapment" and the "back mice phenomenon")
*We have published a review about back mice: you may access a free on line pdf in the following link → Historical Review of Studies on Sacroiliac Fatty Nodules (Recently Termed “Back Mice”) as a Potential Cause of Low Back Pain. Cañis Parera et al. Pain ther (2021).
This is a monologue of 5 minutes in Catalan language. It was part of a contest called “Do you want to know what I investigate?” in November 2018 in Reus. It was organized by the Universtitat Rovira i Virgili and its aim was to promote research’s vocations among youngsters.
Title: back mice or “ratolins a l’esquena”
This is the translation of the monologue:
Please, raise your hands those of you who know someone that has ever had “back pain”.
Many of you, as you can see… since it is considered that 2/3 of the world population suffer or will suffer “back pain” at some point… So it is a very important health problem.
There are some KNOWN causes for “back pain” such as a herniated disk or the fracture of a vertebra.
But you must know that for most of the cases, that is to say 9/10 of “back pains”, WE STILL HAVEN’T GOT A CLUE what the cause is.
We work with a HYPOTHESIS:
Maybe we know so little about this pain… because we have always researched the same parts of the human body: muscles, tendons, ligaments and bones. But we are also made of ANOTHER component…
ALL OF YOU, close your eyes and visualize a slice of “serrano ham”… There is a reddish tissue, this is the muscle tissue… but there is also a white tissue. This is the FATTY tissue, and this is what I’m studying.
The title of my thesis is “Characterization of Fibro-fatty Tissue in the Low Back”.
You may wonder: Why are you studying it, when nobody else does?
Well, anything can start with a little anecdote, and I’ll tell you mine…
One day, when my husband woke up…
Y: I’ve got back pain.
M: Oh, take ibuprofen.
Y: Won’t you see me? Or palpate me?
M: Ooops… let me see you. Is it painful here? Well, here, where it hurts you, there’s a little lump. But it WON’T be serious.
Y: Oh, it WON’T be SERIOUS. I’ve got a painful lump on my back that didn’t let me sleep and it’s NOT SERIOUS!!!!
All of a sudden, I realized… I had palpated these “little painful lumps” before… and I had the feeling that they weren’t serious… BUT I DIDN’T KNOW WHAT THEY WERE… THEY DIDN’T HAVE A NAME… they didn’t talk me about them at the Faculty of Medicine… and I couldn’t find them in my books…
BUT I was sure that other doctors must have palpated them, as I did.
So I DECIDED to do an Internet research!
And I began with Google… I didn’t have a medical word and I typed (in Spanish) “painful lumps in the back”. I found lots of forums where people said: I’ve got a painful lump in my back and my doctor doesn’t know what it is”.
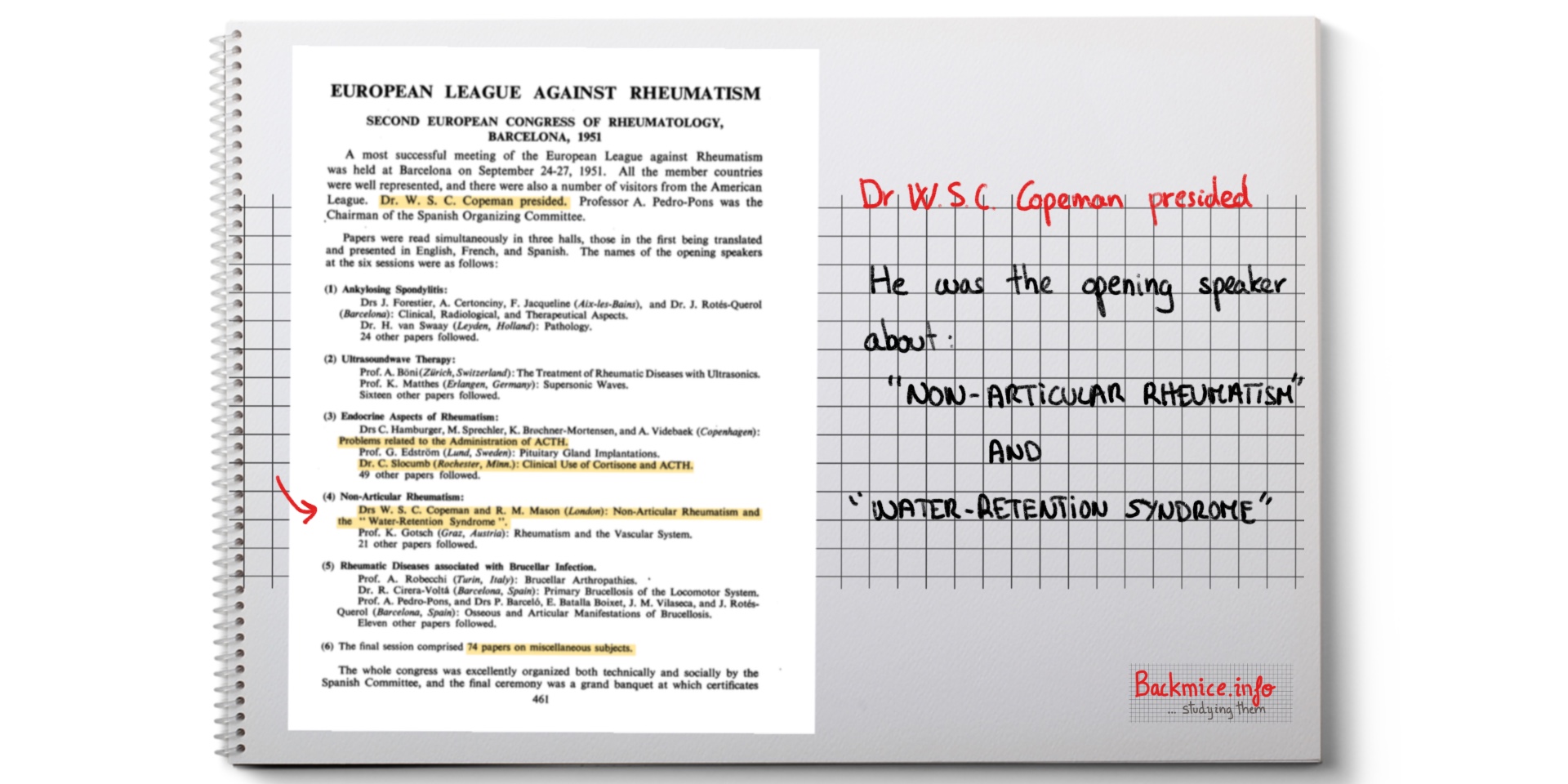
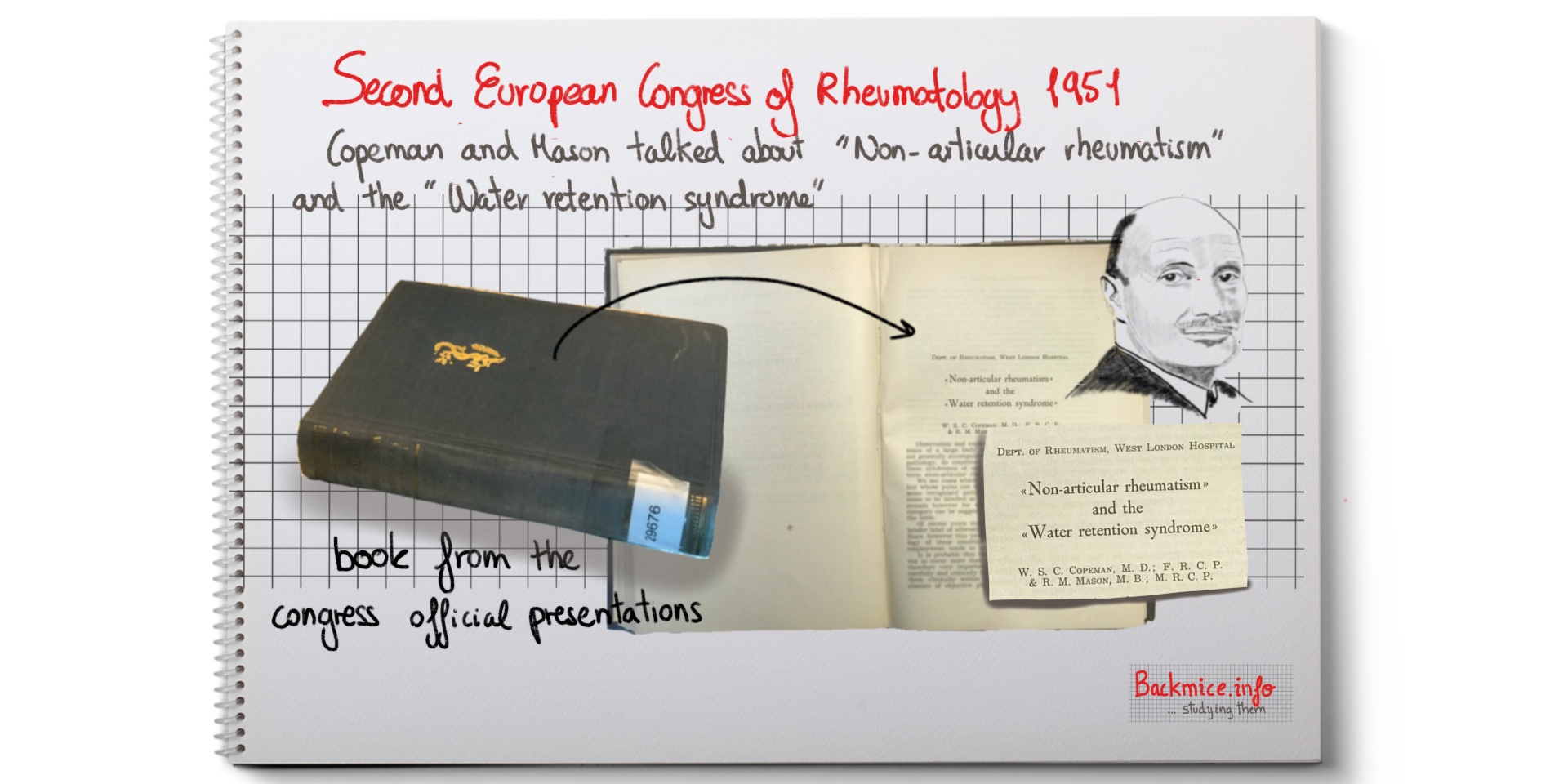
Then I searched in English, pulled the string and… SURPRISINGLY I found lots of information from doctors who, throughout history and in many different parts of the world, had studied these nodules.
Now I’m studying ALL THE scientific ARTICLES and books that have been published, and I have even used Google translator to understand articles In Romanian, Italian or Serbian… I have also created a web page where I upload all the information I find and share it with other researchers…
So, what is the NAME for these nodules? Well, throughout the history of medicine they have been given MANY names… it seems that every person that discovered them gave them a name.
But the funniest name of all –the one that the latest articles use- and my favorite is the name that an American doctor gave them… back in the 90s… “back mice”.
And what do we know about these mysterious nodules?
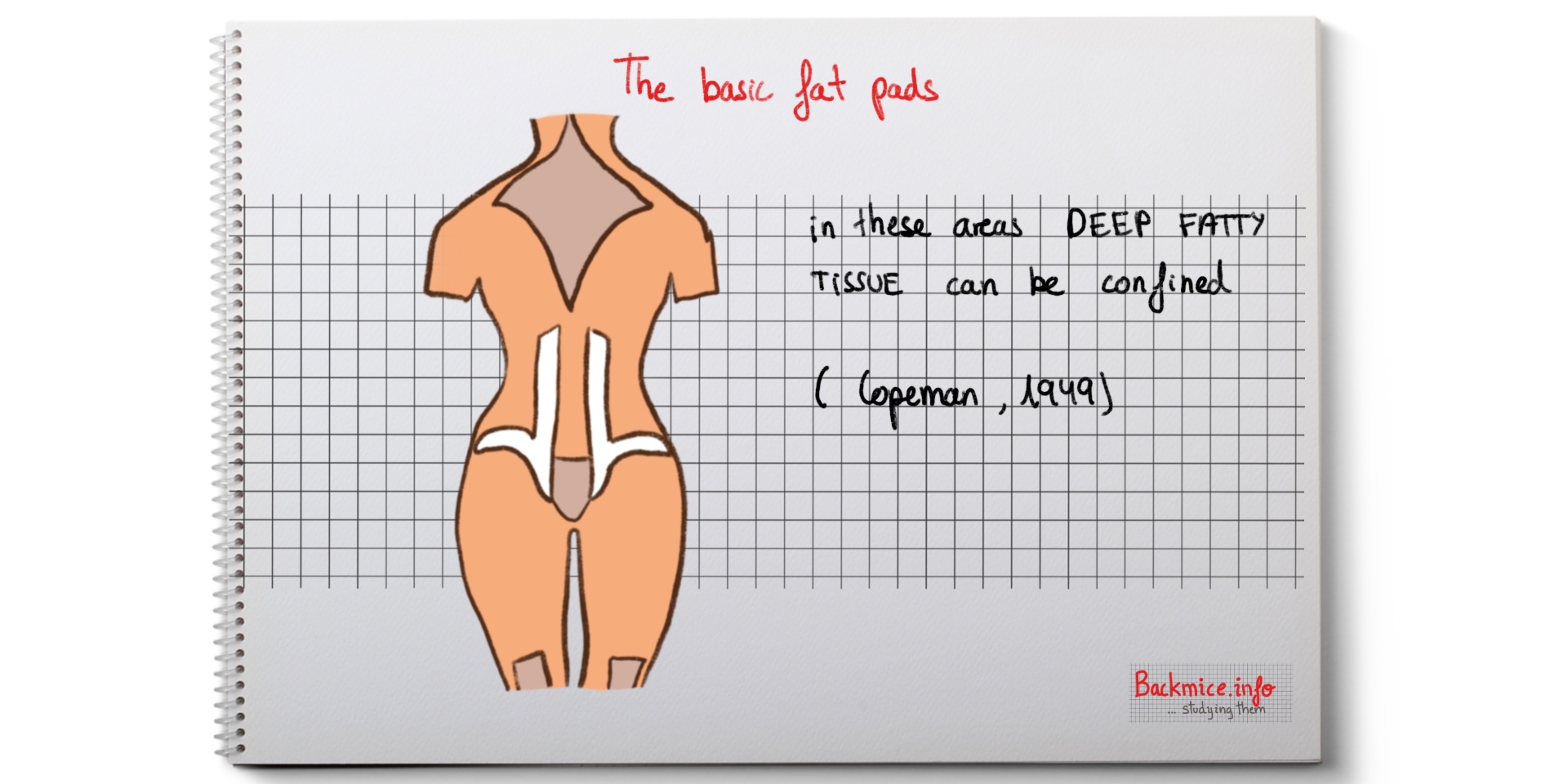
Back mice are nodules of fat, which can be palpated in the DEEP low back, just here, where people put their hands when they have some backache. By the way, it is better to palpate them with some cream on one’s hand and the patient standing.
They have a CAPSULE, so when you palpate them, the skin feels slippery and they seem to be moving and escaping. That’s why they’re called “mice”.
They hurt when they swell. Imagine a ball under your skin that grew bigger and harder.
They can be small, the size of a pea, or big, and the size of a plum.
We have found out many things about “back mice”, but we STILL HAVE many, many questions that need to be answered:
-Why do some people have them and others don’t?
-Why are some of them painful and others are painless?
-Why CAN’T we find this knowledge in our books?
For different reasons, but maybe the fact that we doctors made the mistake to stop palpating patients a long time ago was one of them. Somehow, we used X- rays (where back mice can’t be seen) instead of our HANDS.
Now YOU do! You know more than many doctors do. You know that some little lumps that can be palpated here, in the low back zone, are called BACK MICE, and they sometimes swell and are painful… There’s STILL a lot of work to be done and many questions to be answered. If you are eager to investigate, come on! We’ll keep on studying these nodules that are so intriguing!
Marta Cañis Parera